The Paper of the Month October
01 Oct 2021A new WSA feature highlighting original research in the field of neurology, selected by WSA Editor-in-Chief Gustavo Saposnik.
Editorial
Title: Therapeutic decisions under uncertainty: What is the right thing to do?
Author: Dr. Gustavo Saposnik, EiC, WSA
This article is a commentary on the following
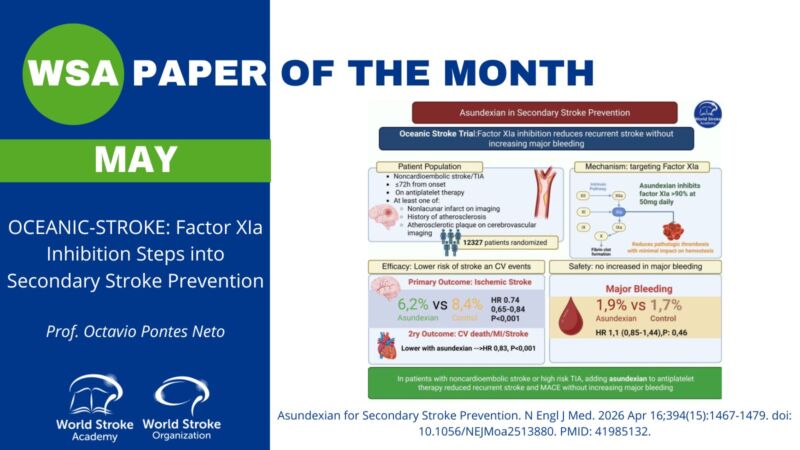
Summary1: In a prospective, randomised, open-label, assessor-masked, parallel-group, pilot phase study conducted at 61 hospitals in the UK, 203 patients with atrial fibrillation (with at least a CHA2DS2-VASc score of 2) and an intracranial hemorrhage (ICH) were randomly assigned to start (n=101) or to avoid (n=102) long-term (over 12 months) oral anticoagulation. The median time was 115 days (IQR 49–265) after the index ICH onset. Participants assigned to start oral anticoagulation (OAC) received either a direct oral anticoagulant or vitamin K antagonist, and the group assigned to avoid oral anticoagulation received usual care (UC; antiplatelet agent or no antithrombotic agent). The planned sample size was 190 participants (one-sided p=0·025, power 90%, allowing for non-adherence) based on a non-inferiority margin of 12% (or adjusted hazard ratio [HR] of 3·2). The primary outcome was a recurrent symptomatic spontaneous ICH.
Oral anticoagulation (OAC) was not non-inferior to avoiding oral anticoagulation (recurrent ICH: 8% OAC vs. 4% UC; adjusted HR 2·42 [95%CI 0·72–8·09]; p=0·152). Serious adverse events occurred in 17 (17%) participants in OAC group and 15 (15%) in the UC group. 22 (22%) patients in the OAC group and 11 (11%) patients in the UC group died during the study.1
Commentary: Clinicians commonly face the challenging question of initiating or continuing OAC for high-risk patients with atrial fibrillation who had a recent ICH.
There is limited supportive evidence about the best choice and timing of anticoagulation after a spontaneous ICH.2, 3 For example, a meta-analysis comprising 5306 ICH patients showed that re-initiation of OAC was associated with a significantly lower risk of thromboembolic complications (pooled relative risk, 0.34; 95% confidence interval, 0.25–0.45).3 Other studies showed no significant reduction in thrombotic events or double risk of bleeding when resuming OAC after any major bleding.2 Similarly, some controversial results were observed on clinical outcomes for the use of antithrombotic agents among patients with ICH.4, 5 A summary of the studies on antithrombotic resumption among patients with ICH can be found at https://www.strokebestpractices.ca/-/media/73bdf8cd90284b979dd2d4ecd8ec3b8b.ashx.
Some scientific organizations provide recommendations based on expert opinion. For example, Thrombosis Canada suggests: i) to restart anticoagulation when hemostasis is achieved, ii) To be aware that prolonged interruption of OAC exposes high-risk patients to an increased risk of thrombotic events, iii) to reassess the appropriateness of drug and dose of anticoagulant based on clinical characteristics such as indication, age, weight and creatinine clearance, iv) To assess co-medications (polypharmacy) that may contribute to bleeding (e.g. concomitant use of ASA, NSAIDs).
The authors SoSTART trial made a step forward to answer this critically relevant clinical question. Unfortunately, we still do not have a clear answer. It appears that re-starting OAC after an ICH is beneficial in decreasing the risk of thrombotic events compared to patients not receiving OAC when warranted. More clinical trials evaluating specific subgroups of patients would be needed to answer this question. A comprehensive review of this topic provides other considerations.6 Meanwhile, we can apply our clinical judgement supported by existing risk scores (CHADS2VASC, HAS-BLED) to provide counselling to patients and their families.6
Resumption of OAC among patients with ICH is a good example of share decision making under uncertainty.7, 8 Gathering information about individual patient’s preferences and their risk tolerance followed by an open discussion about the benefits and risks of OAC in this scenario would facilitate consensus to ameliorate the distress associated with the uncertainty regarding the optimal therapeutic choice.
References
- So SC. Effects of oral anticoagulation for atrial fibrillation after spontaneous intracranial haemorrhage in the UK: a randomised, open-label, assessor-masked, pilot-phase, non-inferiority trial. Lancet Neurol. 2021;20:842-853.
- Little DHW, Sutradhar R, Cerasuolo JO, Perez R, Douketis J, Holbrook A, Paterson JM, Gomes T and Siegal DM. Rates of rebleeding, thrombosis and mortality associated with resumption of anticoagulant therapy after anticoagulant-related bleeding. Canadian Medical Association Journal. 2021;193:E304.
- Murthy SB, Gupta A, Merkler AE, Navi BB, Mandava P, Iadecola C, Sheth KN, Hanley DF, Ziai WC and Kamel H. Restarting Anticoagulant Therapy After Intracranial Hemorrhage. Stroke. 2017;48:1594-1600.
- Baharoglu MI, Coutinho JM, Marquering HA, Majoie CB and Roos YB. Clinical Outcome in Patients With Intracerebral Hemorrhage Stratified by Type of Antithrombotic Therapy. Front Neurol. 2021;12:684476.
- Al-Shahi Salman R, Dennis MS, Sandercock PAG, Sudlow CLM, Wardlaw JM, Whiteley WN, Murray GD, Stephen J, Rodriguez A, Lewis S, Werring DJ and White PM. Effects of Antiplatelet Therapy After Stroke Caused by Intracerebral Hemorrhage: Extended Follow-up of the RESTART Randomized Clinical Trial. JAMA Neurol. 2021.
- Li Y-G and Lip GYH. Anticoagulation Resumption After Intracerebral Hemorrhage. Current atherosclerosis reports. 2018;20:32-32.
- Berger Z. Navigating the unknown: shared decision-making in the face of uncertainty. J Gen Intern Med. 2015;30:675-8.
- Politi MC, Clark MA, Ombao H, Dizon D and Elwyn G. Communicating uncertainty can lead to less decision satisfaction: a necessary cost of involving patients in shared decision making? Health Expect. 2011;14:84-91.
Author Interview
Rustam Al-Shahi Salman, Professor of clinical neurology | Head of the cerebrovascular research group | Clinical director of Edinburgh Clinical Trials Unit at The University of Edinburgh, Honorary consultant neurologist in NHS Lothian
1. WHAT DID YOU SET OUT TO STUDY?
We initiated the Start or STop Anticoagulants Randomised Trial (SoSTART) for survivors of spontaneous intracranial haemorrhage who have atrial fibrillation to establish the feasibility of performing a definitive randomised trial in an acceptable timescale and to estimate whether the risk of recurrent symptomatic spontaneous intracranial haemorrhage after oral anticoagulation is sufficiently low (non-inferior) to justify a definitive randomised trial.
2. WHY THIS TOPIC?
Compared with the general population, survivors of spontaneous (non-traumatic) intracerebral haemorrhage are at higher risk of ischaemic stroke and myocardial infarction, and their risk of all major vascular events is higher still (about 8% per year overall). Atrial fibrillation is present in 14–42% of patients with any type of intracranial haemorrhage, and more than doubles the risk of major vascular events.
3. WHAT WERE THE KEY FINDINGS?
Whether starting oral anticoagulation was non-inferior to avoiding it for people with atrial fibrillation after intracranial haemorrhage was inconclusive, but rates of recurrent intracranial haemorrhage were lower than expected. Furthermore, analyses of three composite secondary outcomes assessing ‘net benefit’ were promising, so the possibility that oral anticoagulation might be superior for preventing symptomatic major vascular events should be investigated in adequately powered randomised trials.
4. HOW MIGHT THESE RESULTS IMPACT CLINICAL PRACTICE?
The directions of the effects and the severities of the outcomes that we have observed can inform discussions with patients and carers in clinical practice, mainly to counsel them about the need for their participation in ongoing randomised trials to resolve this therapeutic dilemma (STATICH [NCT03186729], A3ICH [NCT03243175], ASPIRE [NCT03907046], ENRICH-AF [NCT03950076], and PRESTIGE-AF [NCT03996772]).
5. WHAT SURPRISED YOU MOST?
Although there is a huge amount of research interest in the form of several randomised trials in this area, because oral anticoagulation is a promising intervention, physicians and patients can be reluctant to take part. SoSTART makes it clear that if we are to generate high quality evidence for survivors of intracranial haemorrhage, large numbers of patients must be recruited, so participation needs to be encouraged given the rarity of haemorrhagic stroke compared to ischaemic stroke.
6. WHAT’S NEXT FOR THIS RESEARCH?
Definitive randomised trials appear feasible, justified, and are ongoing, to investigate the effects of oral anticoagulation on major bleeding, any stroke, or any symptomatic major vascular event. Safety monitoring and analysis of ongoing trials should consider the varying severities and frequencies of the outcome events that we observed. Ultimately, a meta-analysis will maximise the precision of estimates of effect both overall as well as in important demographic, clinical, and imaging subgroups as part of a planned collaborative individual participant data meta-analysis, COCROACH (PROSPERO CRD42021246133).
7. IS THERE ANYTHING YOU’D LIKE TO ADD?
There’s a 2-minute video abstract available on our website, which you could link to or embed in your coverage: https://www.ed.ac.uk/clinical-brain-sciences/research/so-start/sostart-news/results-video